Study: Inequity rampant among metro Atlanta hospitals

Two north Georgia hospitals fall among the 50 most segregated in U.S. metropolitan areas, and metro Atlanta tied for the largest number of such hospitals overall, according to a new study by the Lown Institute.
The think tank’s researchers studied 2018 Medicare patient data at more than 3,200 hospitals in U.S. metro areas and compared it with the face of the Medicare-age population surrounding each hospital. That analysis found significant differences in the racial makeup, pointing to hospitals that are not inclusive of their communities.
Such gaps in patient demographics may mean that patients of color are discouraged from showing up to a hospital, or are not being admitted when other patients might be, because of decades of racial inequities in health care, the think tank’s experts said.
But the gaps can also worsen the inequities, particularly if they result in hospitals that serve large number of the poor being swamped with patients, while elite hospitals have manageable and more lucrative patient loads.
“Existing patterns of hospital segregation are deeply rooted, but they must change,” the Institute said in announcing the findings.
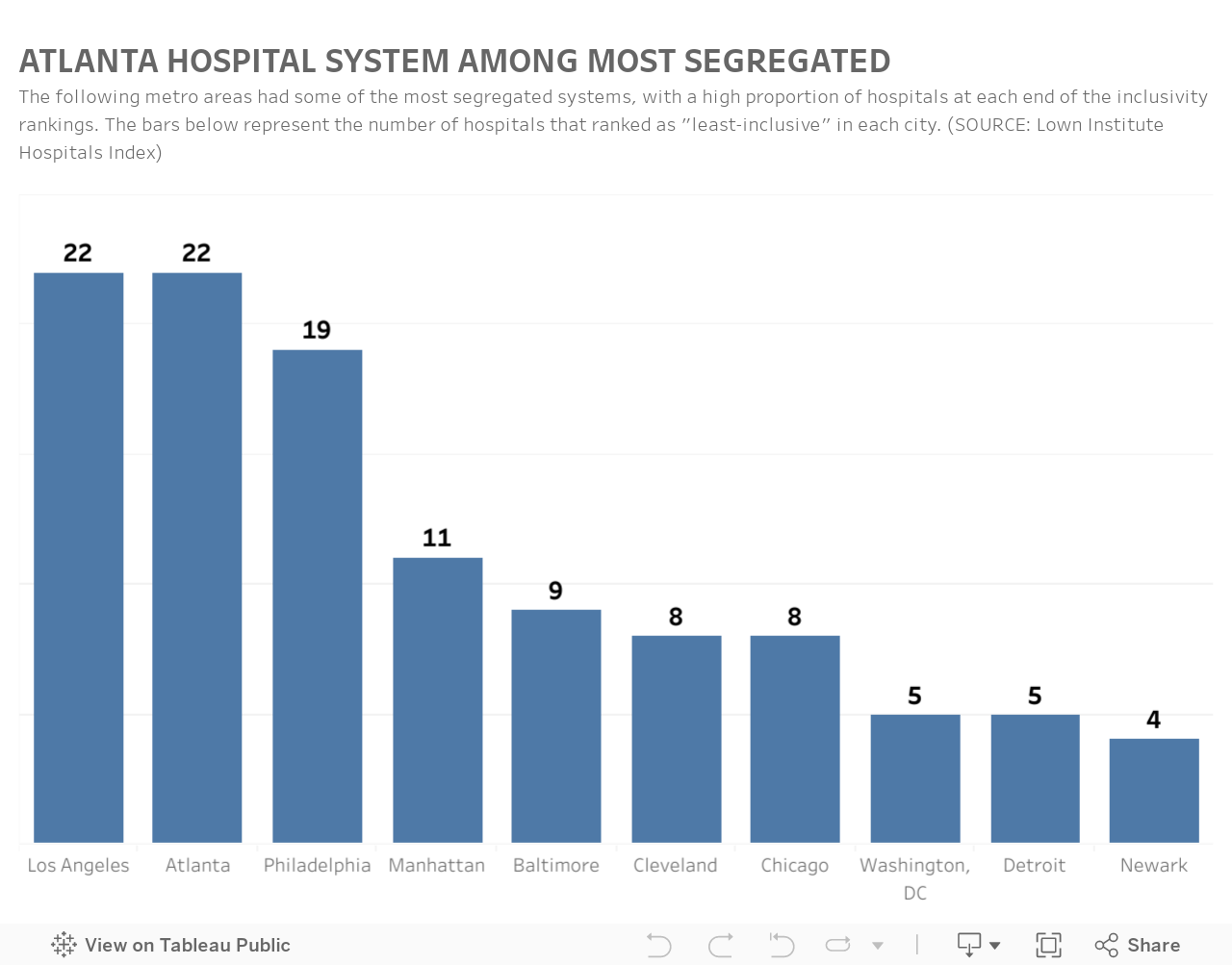
Its analysis found that of 48 hospitals in the greater Atlanta metro area, 22 were “least inclusive,” tying with the Los Angeles area for the highest number among metro areas studied.
Two of the Atlanta-area hospitals —Northside Hospital Cherokee in Canton and CHI Memorial Hospital in Fort Oglethorpe, Catoosa County — were among the top 50 U.S. hospitals where the racial makeup of the Medicare patients was out of step with the race of the surrounding Medicare-age population, the study found.
At the 50 facilities, people of color made up 17% of the patients on average.
At the same time, metro Atlanta also had two of the most racially inclusive hospitals found in the study. Wellstar Atlanta Medical Center and Emory Midtown ranked among the top 50 in the U.S.
At those 50, people of color made up 61% of patients on average.
But where some other metro areas had more of a balance between the number of least and most inclusive hospitals, metro Atlanta had only six on the list of inclusive hospitals. Los Angeles had 14.
The study did not examine hospital quality.
Both Georgia hospitals mentioned in the study’s more segregated list pushed back at the findings, saying they are open to patients of all races.
“Northside is a network of community hospitals, serving all citizens of a very diverse region,” Lee Echols, vice president of the Northside Hospital system, said in a statement. “Our patients at Northside Cherokee reflect the demographics of its community, just as our patients elsewhere reflect those communities. We market our medical services to everyone, and no one is excluded.”
A spokeswoman for CHI Memorial said in a statement that its “mission is to improve the health of the people we serve, especially those who are vulnerable. We provide high-quality, compassionate care to everyone, regardless of race, ethnicity, or ability to pay.”
The Georgia Hospital Association did not provide a comment on the study.
In some of the cities studied, the least and most inclusive hospitals were separated by only blocks. In one example, two hospitals located near each other in New York’s Harlem area served very different populations, with the more elite one serving a population that was more heavily white.
While most all of the hospitals studied are nonprofit, some market their more lucrative services, such as high-tech heart and orthopedic procedures.
Lown Institute officials acknowledged that data was hard to come by, and theirs could have gaps. For example, the data could be skewed in an area with a heavy population of non-citizen people of color: Those people would show up in the census as over 65, but even if they were patients at the hospital they would not be among the Medicare patient load. Medicare does not cover undocumented immigrants
A group of panelists who spoke Tuesday at the Lown Institute’s launch event for the study cited a range of factors that can lead to a disjoint between who a hospital logically could treat and who it does treat.
For example, the panelists said, people of color may have learned from their community or their own experience that their medical complaints are more likely to be rebuffed at one hospital than another.
Panelists also said that patients of color are less likely to have had good health insurance over time, and may be less likely to have built a relationship with a primary care doctor they can see for a possible complaint.
As a result, they may suffer from chronic health conditions, which can be costly to treat.
Dr. Aletha Maybank, chief health equity officer and vice president of the American Medical Association, called for benchmarks to hold practitioners and institutions accountable to equity standards.
“What happens when the patient gets into the healthcare system?” Maybank asked. “Are they going to be referred (for hospital care by doctors who see them initially) in the way that other patients are going to be referred, as black patients? We know the evidence tells us that that is not what happens.”
“As daunting as these challenges are, it’s so important that we are confronting them,” said Harriet Washington, a medical ethicist and panelist who spoke at the study’s launch. “That gives me a lot of hope.”
About the Author

Ariel Hart is a reporter on health care issues. She works on the AJC’s health team and has reported on subjects including the Voting Rights Act and transportation.
