Graham-Cassidy obscures deadlines for other key actions on health care

Nearly one hundred and fifty million dollars to keep Georgia hospitals’ indigent care afloat. Funding for the PeachCare program that along with Medicaid covers about half of Georgia’s kids. Clear answers on Obamacare subsidies that Blue Cross said it needed to keep selling individual plans in metro Atlanta.
Those are some things that Congress has not taken care of — or even, in some cases, clarified its position on — as deadlines and expirations approach at the end of September. That’s this week.
Instead, all eyes in the Senate have been trained on a revival of the plan to repeal and replace Obamacare, which happens to face the same deadline. Even as key votes slipped away Friday afternoon, Senate leadership had still announced no pivot, and weeks of crucial negotiating time remained lost.
The Senate has made nationwide headlines about the tightrope it has walked with the sudden decision to launch full-force back into the repeal debate. Momentous questions affecting one-sixth of the national economy — the health care sector — will be considered and perhaps voted on in the space of days, with no room for revision if it passes on to the House.
But left in the shadows now is yet another ticking clock, counting down on bread-and-butter programs that make the nation’s health care system function.
Ethan James, senior vice president of the Georgia Hospital Association, said lawmakers were right to take care with the bill (known as Graham-Cassidy, after its authors), because of its potential impact. But letting this other funding fall through the cracks, he indicated, would be disastrous.
"There are all of these other things affecting patient access," James said. "DSH (hospital poverty care) cuts are pending. PeachCare is just — I don't think there is enough hyperbole to use for the importance of the CHIP (Children's Health Insurance Program, PeachCare's federal parent) program here in Georgia. … Then the rural extenders," he added, referring to two small programs that help keep 41 rural hospitals running, and are also set to renew — or expire — Sept. 30.
“And yet Graham-Cassidy is sucking the oxygen out.”
High stakes
Defenders of the Senate’s strategy say that if the repeal bill passes, it will take care of many problems that those programs currently do — and also, that Obamacare must be repealed.
Initially, under Graham-Cassidy, Georgia would get a large influx of federal money redirected from other states. In later years, however, the provisions would change dramatically.
U.S. Sen. David Perdue, a Republican, has told The Atlanta Journal-Constitution that he is “all in” on the repeal bill. Asked about funding the current programs, he said that pending federal payment cuts to hospital indigent care are “what we’re trying to avoid.”
“That’s the sense of urgency, because people are hurting out there,” he said, noting that insurance premiums for people who are not indigent are about to increase. “The reality is that Obamacare doesn’t work.”
Insurance providers by county
Alliant
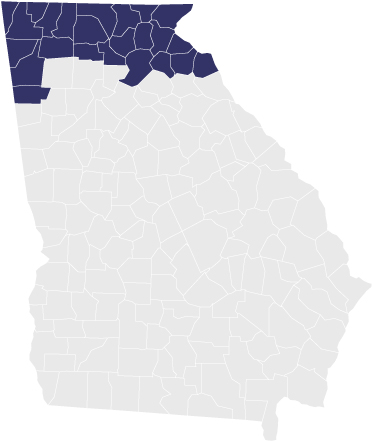
Ambetter
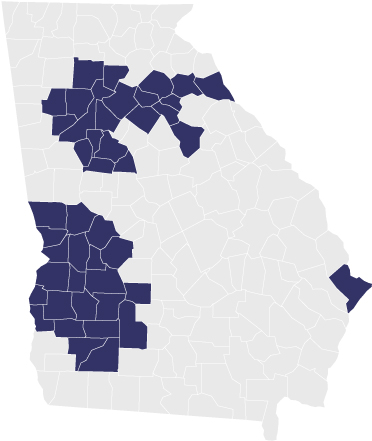
Blue Cross
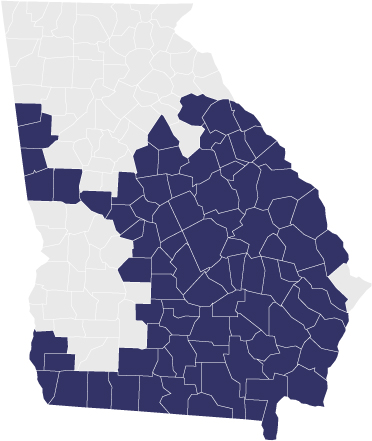
Kaiser
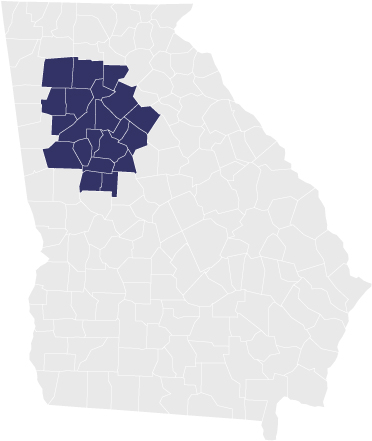
Source: Georgia Department of Insurance
Kevin Bierschenk, the CEO of Dodge County Hospital, has no appetite to gamble on the future impact of the bill, which some estimates have said would eventually decrease Georgia’s expected funding for the poor. And in the meantime, he wants some focus brought to the funding sources that keep rural hospitals like his going.
Bierschenk says that his facility survives and employs 200 with money from an array of programs that are set to expire Saturday. It receives funding for hospitals that treat a disproportionate share of indigent patients (known technically as DSH, for Disproportionate-Share Hospital); treats patients on PeachCare (which is the Georgia iteration of CHIP); and also receives payments for smaller rural hospitals (known as Low-Volume Adjustment funding). The Low-Volume Adjustments and another fund together send about $11 million to 41 rural Georgia hospitals, according to the state’s hospital association. It may not seem like much, Bierschenk said, but the $445,000 his hospital gets from it is close to half its bottom line.
Care has gotten remarkably expensive to deliver, he said. And it's a grave misconception that most people who walk into a facility have private insurance or the personal means to pay. Employer insurance now covers fewer than half of all Georgians. And Medicaid and Medicare are barely break-even, sometimes not even that.
If Congress doesn’t attend to the mundane pots of money that make medical providers’ checks clear, he said, there will be consequences. Like rural hospitals closing, unless county taxpayers decide to take up the slack.
“I think back to the politics, it’s impacting everybody’s lives,” Bierschenk said. “We’re letting politics control our health care.”
At least one piece of that funding, CHIP, is widely popular across party lines, and few observers think Congress would let it go away. It covers about 132,000 children in Georgia whose families make too much money to be on Medicaid but still don’t make enough to buy private insurance.
The top Republican and Democrat on the Senate Finance Committee struck a five-year agreement to renew the popular program earlier this month. But no announcement has been made on when the panel will consider the bill or lawmakers will debate the measure on the Senate floor.
Two Senate aides told the AJC that all other health care legislation besides the repeal bill was unofficially placed on hold until after Graham-Cassidy is resolved, a notion the Republican leadership disputes.
The situation is even more precarious for DSH, which will see cuts starting on Oct. 1 unless Congress steps in. Cuts to Georgia hospitals for the care of the poor are currently scheduled to increase over several years to approximately $149 million annually, with Grady Memorial Hospital alone losing out on perhaps $11 million just next year.
There is no legislation that has been introduced to delay or cancel the upcoming cuts, which Congress has done in the past.
U.S. Sen. Johnny Isakson, a Republican member of the Senate Finance Committee, which has jurisdiction over the issue, said he has an amendment he’s been looking to attach to other legislation that Congress must pass before Oct. 1 that would ward off the cuts. But he’s been tight-lipped about what he’s been trying to attach it to. He’s being backed by Perdue, but the two have yet to be successful.
“Regardless of whether or not the Senate passes health care legislation, ensuring that Georgia’s charity hospitals continue to have the resources they need is a top priority for Senator Isakson,” said Amanda Maddox, a spokeswoman for Isakson.
And then there are patients who get their insurance on the Affordable Care Act’s exchange market. They’re about to lose options because some companies in Georgia are pulling back from some counties and all are raising rates. Many have named uncertainty surrounding certain federal subsidies as a reason.
Some in Washington hoped to address that — with bipartisan cooperation, no less.
Buoyant headlines greeted an effort led by Republican U.S. Sen. Lamar Alexander to hold hearings to address the subsidies, known as Cost-Sharing Reductions, and stabilize the individual insurance market. The subsidies are used to make out-of-pocket costs for Obamacare customers more affordable, but GOP leaders in the House and the White House have called them into question, and most agree the way to deliver certainty is for Congress to decide whether to appropriate the money. Blue Cross Blue Shield of Georgia specifically mentioned the uncertainty surrounding those subsidies when it announced plans to pull out of metro Atlanta's individual health insurance market. Blue Cross and other companies will finalize their plans for next year on Wednesday.
But in the wake of the splashier legislation this week, Alexander said he’s giving up.
Does it have the votes?
Whether the Senate can conclude its dealings on the repeal legislation by its Sept. 30 deadline is a question in itself. After that, the bill can no longer pass without Democratic support. But Democrats say they want to fix Obamacare, not help repeal it.
As with the infamous government shutdowns, the official deadlines to renew a program may not mean that the money and services would disappear that day. PeachCare, for example, is estimated to have funding until about March or April.
And some advocates cautioned against hysteria about the bill.
“We feel like it’s better than the status quo,” said Kelly McCutchen, the CEO of the free-market Georgia Public Policy Foundation. “From a timing perspective, it’s not like we haven’t been talking about this for six months or more.”
McCutchen believes that Health and Human Services Secretary Tom Price, a conservative Georgia Republican, will use his authority under the repeal bill to give the state an even bigger increase in federal money than he has to. He also believes that other analyses predicting deep cuts for Georgia Medicaid in the bill’s outer years have been overly pessimistic in their assumptions; McCutchen believes Medicaid funding for the state could actually continue to outpace what the state expects now.
“In the long run we are going to have more funds to address health care issues in Georgia than we would without the bill, with less strings attached,” McCutchen said.
And more than that, “We think it would be a great failure to come out of this whole 10-month discussion with no bill.”
As senators left town last week, no one knew for sure how many votes GOP leaders had for the bill. Senate Majority Leader Mitch McConnell left an assurance of drama in his wake, saying through his office not just that deliberations would continue when the senators returned but that he intended to bring it up for a vote. But on Friday, U.S. Sen. John McCain, R-Ariz., came out against it, leaving Graham-Cassidy teetering.
Some publications said McConnell left himself wiggle room to back out of a public vote, though, if he knows it won’t win.
Democrats pounced on the last-minute timing with the stakes so high.
U.S. Rep. Hank Johnson, D-Lithonia, said that the repeal bill was “the worst piece of legislation that has come down the pipe yet.” He said Congress would want to reauthorize the indigent hospital care and PeachCare programs. “Hopefully, Republicans in Congress can walk and chew bubble gum on that issue,” he said.
Some outside experts were also wary of the solidity of the policy.
Timothy Jost, a law professor and health law expert at Washington and Lee University in Virginia, was deeply concerned about whether the 50 states have the administrative and political wherewithal to perform all the new functions the repeal bill would give them should it pass both chambers of Congress.
“It just seems to me that this is just walking off a cliff,” Jost said. “Whether they can do it or not, I think some Republicans are desperate to pass absolutely anything. They don’t care what it is. They aren’t even interested in reading it.”
But putting aside whether the legislation is good or bad, few had good things to say about the path to get there.
“Boy, I sure wouldn’t want to be trying to figure out at the state level how to plan my budget, how to plan coverage and how to work with the providers and the individuals in my state,” Diane Rowland, executive vice president of the Kaiser Family Foundation, a nonpartisan health care research organization, said in a conversation about Georgia’s predicament. “For people who like to do things in a strategic and planned way, this is one of the most chaotic health policy environments that I’ve ever seen.”
Programs facing deadlines
CHIP (PeachCare for Kids)
CHIP, or S-CHIP, in Georgia is known as PeachCare for Kids. The program, approved by the Georgia Legislature in 1998 and funded mostly by the state and federal governments, insures children whose families make too much for the kids to be on Medicaid but make less than 2.5 times the poverty level. Just the kids are insured, until they hit their 19th birthday. PeachCare has about 132,000 patients on its rolls now, and Medicaid and CHIP together insure about half of Georgia’s children.
DSH (Disproportionate-Share Hospital payments)
These payments go to hospitals that care for a disproportionate share of patients who are unable to pay. Grady Memorial Hospital is the main one in Georgia, but many others benefit from the money. Under Obamacare, DSH funding was scheduled to wind down as states expanded Medicaid. But states such as Georgia decided not to expand Medicaid under Obamacare, so the funding gap created by winding down DSH would yawn unfilled if Congress doesn’t act. Georgia’s funding is currently scheduled to decline by $200 million or so by 2025.
CSR (Cost-Sharing Reductions)
These subsidies are funneled to insurers by the administration, to offset the out-of-pocket costs of lower-income Obamacare policyholders. GOP members of the U.S. House sued, saying Congress had to greenlight such spending, not the administration. President Donald Trump has continued to make the payments month to month, but he has made noises about stopping them. Insurance companies have said they can’t do business under such uncertainty. Blue Cross Blue Shield of Georgia cited the uncertainty over these subsidies in pulling out of the individual market in Georgia’s metro areas and proposing to raise rates an average of 40.6 percent next year. Other companies have also proposed to raise rates, and experts say they’re pricing in the subsidy uncertainty. Those decisions will be finalized with regulators on Wednesday.
So-called rural extenders:
“Rural extenders” is a nickname some give to Medicare Dependent Hospital funding and Low-Volume Adjustments. The Low-Volume Adjustments go to hospitals that are 15 miles away from another hospital and have a low volume of certain kinds of patients. The total annual loss to Georgia hospitals if cuts are allowed to take effect to the two programs would be $11.7 million, according to the Georgia Hospital Association.
About the Authors

Ariel Hart is a reporter on health care issues. She works on the AJC’s health team and has reported on subjects including the Voting Rights Act and transportation.

Tamar Hallerman is an award-winning senior reporter for The Atlanta Journal-Constitution. She covers the Fulton County election interference case and co-hosts the Breakdown podcast.


